Liposomal Vitamin C Uses
There's little doubt that vitamin C is of great benefit to the human body. However, how you consume vitamin C makes a huge difference in the amount your body is able to absorb and use (a feature of all supplements called "bioavailability").
Liposomal (or pro-liposomal) vitamin C is a groundbreaking option for high-dose vitamin C.
Between 14-30% of the vitamin C consumed in supplement form is actually absorbed by the body. ( Source 1) That number can vary greatly depending on your own vitamin C needs and the type of supplements you take. Consuming five servings of raw foods high in vitamin C per day, such as berries, kiwi, broccoli and citrus, will provide adequate vitamin C. Adding supplemental vitamin C in the form of ascorbic acid, the equivalent form of vitamin C found naturally in foods, will increase blood levels further, but natural absorption of vitamin C above the intake of about 200 mg decreases sharply with increasing doses by as much as 50%. ( Source 2) This may be because our bodies use certain transporters of vitamin C in the small intestine called Sodium-Dependent Vitamin C Transporters (SVCT -1) which will absorb efficiently only up to a certain point and this absorption is regulated by our bodies depending on the level of vitamin C in plasma (blood). In addition, any excess absorbed vitamin C is destined to be excreted in urine to maintain a small tight control on plasma concentrations. This is where liposomal vitamin C has an advantage.
Liposomes are phospholipid containing microscopic spheres that carry vitamin C at their core. Their absorption does not depend on vitamin C transporters like SVCT-1 but rather on the direct fusion of the liposome with the small intestinal cells resulting in the direct intracellular release of the vitamin C which eventually ends up into the blood circulation.
Not only does liposomal vitamin C have a substantially higher absorption rate than conventional vitamin C supplements, but it also comes with its own host of health benefits. This is due to the phospholipids used to surround, or encapsulate, the vitamin C — the very mechanism that allows it to bypass the slow vitamin C transporters present in the gut. In this article, I discuss the definition of liposomes and how to choose the best liposomal supplement and potential side effects.
What are liposomes?
Liposomes are actually similar to cells. The same phospholipids that makeup cell membranes also make up the outer shell of liposomes. The inner and outer walls of the liposome are made up of phospholipids, the most common being phosphatidylcholine, to create a lipid bilayer. A double layer of phospholipids (phospholipid bilayer) creates a sphere around an aqueous (water-containing) component, such as dissolved vitamin C.
Because the liposomes' outer shells imitate our cell membranes, liposomes can "fuse" with certain cells upon contact, delivering the liposome's content to the cell.
This is the scientific advantage of the liposomal delivery system.
Liposomes were discovered in the 1960s. This novel delivery system offers a targeted method to get nutrients into the bloodstream without being destroyed by the digestive enzymes and acid found in the digestive tract and stomach respectively.
What is liposomal vitamin C?
In the case of liposomal vitamin C, these phospholipids encapsulate vitamin C at their core.
As mentioned above, liposomes are thought to fuse with the cells responsible for absorbing nutrients making up the gut lining called enterocytes. Because they bypass the normal mechanism of absorbing vitamin C through slow vitamin C receptors type 1 (sodium-dependent vitamin C receptors SCVT 1), the bioavailability is much higher than standard vitamin C supplements. ( Source 3 )
Taking a liposomal form of vitamin C is much more effective and efficient than traditional methods of vitamin C supplementation in terms of absorption.
5 Benefits of Liposomal Vitamin C
Taking standard vitamin C (ascorbic acid) offers several benefits to the human body. These benefits may be magnified when taking liposomal C.
1. Bioavailability
The best-understood advantage is that liposomal vitamin C has a much higher bioavailability than standard vitamin C.
Bioavailable simply means how well vitamin C absorbs into your system. As we already mentioned liposomal vitamin C supplement allows your small intestine to absorb more of the nutrient than a standard vitamin C supplement.
A 2016 study in 11 human subjects found that vitamin C encapsulated in liposomes increased vitamin C levels in the blood by substantially compared to an un-encapsulated (non-liposomal) supplement at the same dose (4 grams). ( Source 4 )
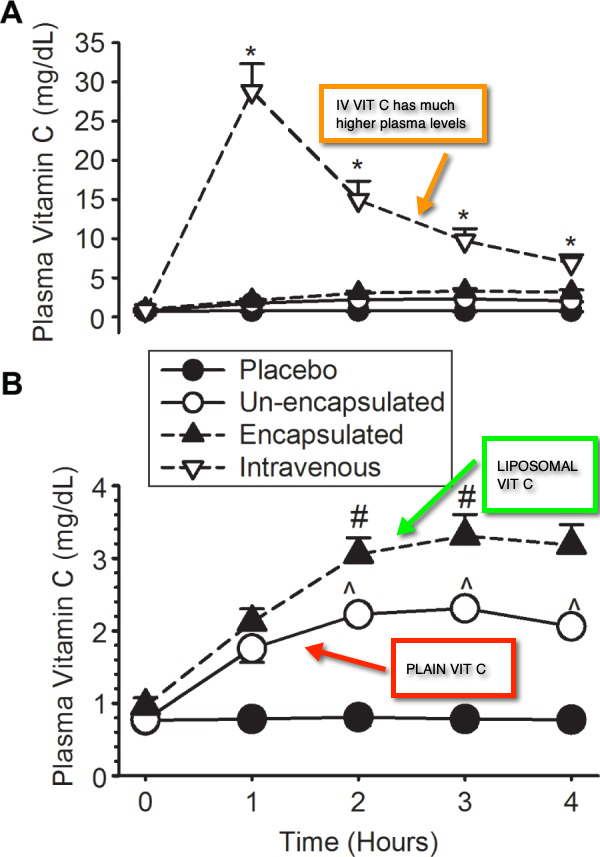
Liposomal vitamin C's bioavailability is only outstripped by intravenous (IV) vitamin C. IV vitamin C which has 100% bioavailability by definition, but is much more invasive, as it requires a needle insertion, a specially trained facility, and 1-3 hours of time for the slow infusion.
High doses of IV vitamin C are used most frequently in conjunction with cancer treatment and provide a pro-oxidant effect which can ONLY be achieved with very high IV doses of vitamin C. The pro-oxidant effect of high dose IV vitamin C is very different than that of low doses of vitamin C which provide anti-oxidant activity.
2. Heart and Brain Health
Vitamin C intake (via diet or supplements) may decrease the risk of cardiovascular disease by about 25%, according to a 2004 analysis published in The American Journal of Clinical Nutrition . ( Source 5 )
Any form of vitamin C supplement improves endothelial function, as well as ejection fraction. ( Source 6 )
Endothelial function involves the contraction and relaxation of blood vessels, enzymatic release to manage blood clotting, immunity, and platelet adhesion. Ejection fraction defines "the percentage of blood that is pumped (or ejected) out of the ventricles" when the heart contracts on every beat.
Together, these results suggest that vitamin C may play an important part in the prevention of cardiovascular disease and the improvement of heart health.
After a stroke or heart attack, it's important to heal the tissues damaged by the lack of oxygen. Once blood flow is restored, the reoxygenation of previously oxygen-deprived cells leads to dtissue damage called "reperfusion injury" which is accompanied by "excessive generation of free radicals". ( Source 7)
When delivered intravenously, vitamin C is a potent antioxidant that can counteract and neutralize free radicals that cause the oxidative stress caused by reperfusion. ( Source 8 )
In one animal study, liposomal vitamin C prevented brain tissue damage from reperfusion when administered before blood flow was restricted. ( Source 9 )
Although blood levels achieved by IV infused vitamin C are much higher than liposomal vitamin C, one study observed that liposomal vitamin C was nearly as effective as IV vitamin C at preventing tissue damage during reperfusion. The research was conducted in 11 subjects who had temporary obstruction of blood flow to their arms blood flow by tourniquet. ( Source 4 )
3. Cancer
Intravenous vitamin C can be used in high doses to fight cancer in tandem with traditional chemotherapy. It may not eradicate cancer on its own, but it can definitely improve the quality of life, increasing energy and mood for many cancer patients.
On a case by case basis, IV vitamin C can even induce regression of cancer. A 2014 review recounts several reports of remission when using IV vitamin C with chemotherapy. ( Source 10 )
However, one should not rely on IV vitamin C to induce remission or treat cancer on it's own, as these cases are isolated at best. Vitamin C can however be a great adjuvant (helper) to traditional cancer treatment.
Liposomal vitamin C has not been specifically tested in human subjects with cancer. Many cancer patients receiving IV vitamin C, however, also use liposomal vitamin C in high doses between IV treatments. After receiving a high dose of IV vitamin C, it is not uncommon for blood levels to drop below normal in the days after the infusion (trough levels). Therefore, it's highly recommended to increase oral intake levels of vitamin C between IV vitamin C infusions especially to prevent low rebound trough plasma levels of vitamin C.
4. Collagen Production
Collagen is the most abundant protein in our bodies, however our own natural collagen production slows around the age of 25. Vitamin C is a cofactor in the enzymes that produce collagen, meaning it is necessary to the function and health of your bones, blood vessels, and joints where collagen abounds. ( Source 11 ). When vitamin C levels run low, such as in times of stress, infection, chronic illness (i.e. diabetes, autoimmune illness which generate high levels of free radicals and oxidative stress), less of it is available for collagen production. Since collagen is the structural protein that holds us together, this can manifest as weaker joints, tendons, blood vessels and connective tissue. More superficially, weaker collagen can manifest as sagging skin with more wrinkles.
5. Oxidative Stress
In general, some level of oxidative stress occurs within every living thing. As a 2006 review puts it:
"There is increasing evidence connecting oxidative stress with a variety of pathological conditions including cancer, cardiovascular diseases, chronic inflammatory disease, post-ischaemic organ injury, diabetes mellitus, xenobiotic/drug toxicity, and rheumatoid arthritis." ( Source 12 )
Vitamin C is a potent antioxidant and is found in generous quantities within the human body. ( Source 13 )
Is liposomal vitamin C truly effective?
There has been a lot of scrutiny of liposomal vitamin C.
One of the most frequently asked questions about liposomal supplements is: Is liposomal vitamin C a "hoax"?
True liposomal or pro-liposomal supplements are non-toxic and can greatly increase your body's ability to absorb the nutrients they incorporate. Because of extensive equipment and technology needed to manufacture them, liposomal supplements tend to be more expensive than conventional vitamin C but they can deliver superior absorption. However there is great variability between products and a little bit of homework and knowledge helps.
How do we know which products are "true" and effective liposomal vitamin C?
As opposed to the term "liposome", the term "liposomal" is unfortunately not well defined. Many products take advantage of this absence of "liposomal" definition.
A "liposome" is a spherical structure made out of a shell formed by phospholipids and surrounded by water. At the center of a "liposome" is usually a main ingredient, like vitamin C or glutathione, also suspended in water.
"Liposomal" on the other hand does not mean "liposome" — these terms are not one and the same even though they do sound similar. The term liposomal is (sometimes) loosely used to only mean "containing fat". So products containing just fat (lipid) and vitamin C mixed together can sometimes be called "liposomal".
The usual lipid that forms liposomes is a "phospholipid". Phosphatidylcholine is the most abundant phospholipid and is the main building block of cell walls as well as the main constituent of the outer shell of liposomes. However the lipid form that some supplements use is not a phospholipid, and can be simply be in the form of a fatty acid which is not as effective.
Products using fatty acids may be labelled "liposomal" vitamin C but might never result in formed liposomes, even when exposed to water because the vitamin C is simply covalently bound to a fatty acid.
The "Fat Soluble" Vitamin C Ester Myth
A perfect example of a product taking advantage of the "liposomal" term is a type of vitamin C a vitamin C ester . Usually labeled as "fat soluble" vitamin C, esters like Ascorbyl Palmitate are marketed as a "liposomal" but will never result in forming an actual "liposome".
Here are some important facts about "fat soluble" Ascorbyl Palmitate:
- Ascorbyl palmitate is not found in nature. It is SYNTHETIC, made by combining palmitate (an ester, fat) with vitamin C (Ascorbic Acid).
- Ascorbyl palmitate is used as a "FOOD PRESERVATIVE" to extend the shelf life of certain foods, medications, and cosmetics.
- Ascorbyl Palmitate is also known as "Cetyl Ascorbate"....(two different names for the same compound)
- Ascorbyl Palmitate is ONLY 42.5% VITAMIN C
- Products that claim "1600 mg Liposomal Vitamin C" using Ascorbyl Palmitate ONLY PROVIDE 680 mg of actual vitamin C (Ascorbic Acid)
This last point is very important. Because Ascorbyl Palmitate is made by combining vitamin C (Ascorbic Acid) to Palmitate (a fat), less than half of it is true vitamin C ! (source 20, source 21).
Ascorbyl Oleate is another vitamin C ester very similar to the Ascorbyl Palmitate compound, binding Oleate (another fat) to ascorbic acid.
Ester forms of vitamin C, like Ascorbyl Palmitate, are easily digested after oral ingestion by enzymes in the small intestine which cleave the bond immediately releasing just plain vitamin C (ascorbic acid molecule) and the ester, in this case palmitate, before any absorption can take place.
When this digestion happens, plain vitamin C is released from the ester andno improved absorption occurs when compared to a standard vitamin C supplement. ( source 15, source 16 ). The bioavailability of fat soluble vitamin C esters is essentially identical to plain vitamin C (Ascorbic Acid) alone. ( Source 18 )
The esters used may even have a negative impact, depending on the ingredient itself.
Unlike natural vitamin C (Ascorbic Acid), Ascorbyl Palmitate may actually be toxic to skin cells damaged by UV exposure according to one study. ( Source 17 )
The bottom line is this: These "Fat Soluble" forms of vitamin C (ascorbyl palmitate, alscorbyl oleate, cetyl ascorbate), are rapidly digested before any absorption takes place, releasing plain vitamin C in your small intestine. Adding to the deception, "Fat Soluble" Vitamin C CONTAINS LESS THAN HALF actual vitamin C (Ascorbic Acid)!
Unfortunately few people know this, results in unassuming customers paying top dollar for a product that is not much different than a standard vitamin C capsule or powder but has the term "liposomal" attached to it.
Because these forms are inexpensive to make they typically have lower prices, yet they tout very high doses per serving such as 1200-1800 mg of vitamin C.
So, to answer the question: Liposomal vitamin C is not a "hoax", but not all products labeled liposomal vitamin C truly offer the same benefits, especially those selling "Fat Soluble" vitamin C esters.
How to Choose the Best Liposomal Vitamin C Supplement
Several brands offer liposomal vitamin C supplements. Which vitamin liposomal vitamin C supplement is the best?
There are two basic types of liposomal supplements that have to do with "liposome" formation. The first is an already formed liposome vitamin C and, while the other is a pro-liposome. A pro-liposome is chemically bound vitamin C and contains phospholipids in a manner which will result in a liposome formation in the presence of water at body temperature.
The simplest way to tell if a product is a formed liposome is if the ingredients include water. If water is in the ingredients, you are likely dealing with formed liposomes. If not, you are looking at a pro-liposome. Make sure however that both contain phospholipids like phosphatidylcholine (derived from lecithin).
A pro-liposome has the potential to become a liposome when exposed to water, forcing the phospholipids to immediately congregate by natural hydrophobic forces into a bi-layer as described above.
In the form of a pro-liposomal powder, the vitamin C is surrounded (conjugated) by a layer of phospholipids and other fats in a special technical process that can greatly vary in effectiveness. How well this proprietary process of binding the lipids to the vitamin C occurs is key, because if the lipids and the vitamin C are only mixed together (not bound), the formation of liposomes with vitamin C inside will be sporadic at best as the vitamin C can just disperse away separately from the lipids.
Liquid pro-liposomes use lipids (fats) and vitamin C. Based on proprietary manufacturing techniques, these lipids will form liposomes around the main ingredient when they are exposed to water and correct temperature conditions, as are found the environment of the small intestine.
The newly formed liposomes can then be absorbed by the intestinal walls, delivered to and processed by the liver, and released into systemic circulation.
To reiterate: all "liposome" formulations (formed liposomes and pro-liposomes) utilize phospholipids, phosphatidylcholine, lecithin as the fatty agent to form liposomes.
Unfortunately, many vitamin C supplements labeled "liposomal" are, in fact, unable to hold the lipid ingredient and vitamin C together when exposed to water in the small intestine.
Make sure the vitamin C is well-sourced. A good liposomal vitamin C supplement should be non-GMO and preferably use phospholipids derived from sunflower lecithin.
Some customers even insist on knowing that the origin of vitamin C is non-Chinese, but this is a personal preference.
If this is important to you, then look for Quali-C brand vitamin C sourced and made in Scotland from non-GMO European origin corn.
Obviously a liposomal vitamin C that also offers a satisfaction guarantee with a full refund is a major plus.
To summarize: Avoid the gimmicks and purchase a high-quality liposomal supplement by following these steps:
- Choose a formed liposomal or a well made pro-liposomal supplement that contains vitamin C and a phospholipids like phosphatidylcholine. Avoid vitamin C esters "lipid soluble" vitamin C like include ascorbyl palmitate, ascorbyl oleate, or cetyl ascorbate as they may offer little if any advantage over regular vitamin C
- Look for the source of vitamin C. While most brand use Chinese vitamin C, Quali-C is a brand of vitamin C manufactured in Scotland using non-GMO European sourced corn
- Ensure the supplement is non-GMO and soy-, gluten-, and dairy free.
Dosage of Liposomal Vitamin C
The National Institute of Health advises men and women to never take more than 2,000 milligrams of vitamin C dietary supplement each day.
For specific health issues, a higher dose may be warranted. The Linus Pauling Center recommends a dose of 2,000 milligrams per day, which is generally very safe and can account for the poorer absorption capacity in some individuals. People who may benefit most from this high dose include the elderly and smokers, who also have an increased need for vitamin C.
Generally, 1000-2000 mg/day should afford you the general health benefits of vitamin C:
- Immunity
- Brain health
- Collagen production
- Cardiovascular protection
- Energy production
- Increased antioxidant presence
4,000 milligrams of liposomal vitamin C has been used to protect against the oxidative damage that can happen post-heart attack or stroke due to reperfusion.
While these results are very promising, I suggest stying at around the 2,000 milligram threshold as a daily maintenance dose, unless a healthcare practitioner advises you to take a higher amount, or you have increased levels of oxidative stress from chronic illness or acute infection which require higher doses.
Liposomal Vitamin C Side Effects:
Although a high dose of vitamin C may not technically be "toxic", it may cause side effects like nausea or diarrhea.
Drug Interactions
Vitamin C interacts with certain drugs or nutrients.
ADD and ADHD medications utilize amphetamines. Vitamin C may weaken the effect of amphetamine-based drugs by limiting their effect, although this result has not been reproduced in human subjects. ( Source 19 )
In Summary
- Liposomal vitamin C is a revolutionary approach to introducing vitamin C into your system.
- Liposomes use a phospholipid bilayer formed around water and, in this case, vitamin C. The outer casing protects the nutrient inside from damage that might otherwise occur during normal digestion.
- The absorption of liposomal vitamin C is significantly higher than that of a standard vitamin C supplement.
- Benefits of liposomal vitamin C include increased bioavailability, cardiovascular support, skin health, improved collagen production, and reduced oxidative stress throughout the body.
- While many supplements are labeled as "liposomal," some of these use esters of vitamin C (ascorbyl palmitate, ascorbyl oleate, and/or cetyl ascorbate) that do not actually increase the bioavailability of vitamin C and are not going to result in formation of a liposome.
- Standard doses of vitamin C are between 200-1,000 mg/day. We recommend 2000 mg per day for most adults.

Sources
- Yung, S., Mayersohn, M., & Robinson, J. B. (1982). Ascorbic acid absorption in humans: a comparison among several dosage forms. Journal of pharmaceutical sciences, 71 (3), 282-285. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/7069582
- National Institutes of Health: Office of Dietary Supplements. (2018). Vitamin C: Fact Sheet for Health Professionals. Retrieved from: https://ods.od.nih.gov/factsheets/VitaminC-HealthProfessional/
- Rivas, C. I., Zuniga, F. A., Salas-Burgos, A., Mardones, L., Ormazabal, V., & Vera, J. C. (2008). Vitamin C transporters. Journal of physiology and biochemistry, 64 (4), 357-375. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/19391462
- Davis, J. L., Paris, H. L., Beals, J. W., Binns, S. E., Giordano, G. R., Scalzo, R. L., ... & Bell, C. (2016). Liposomal-encapsulated ascorbic acid: Influence on vitamin C bioavailability and capacity to protect against ischemia–reperfusion injury. Nutrition and metabolic insights , 9 , NMI-S39764. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4915787/
- Knekt, P., Ritz, J., Pereira, M. A., O'Reilly, E. J., Augustsson, K., Fraser, G. E., ... & Pietinen, P. (2004). Antioxidant vitamins and coronary heart disease risk: a pooled analysis of 9 cohorts. The American journal of clinical nutrition , 80 (6), 1508-1520. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/15585762
- Ashor, A. W., Lara, J., Mathers, J. C., & Siervo, M. (2014). Effect of vitamin C on endothelial function in health and disease: a systematic review and meta-analysis of randomised controlled trials. Atherosclerosis , 235 (1), 9-20. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/24792921
- Nour, M., Scalzo, F., & Liebeskind, D. S. (2012). Ischemia-reperfusion injury in stroke. Interventional neurology , 1 (3-4), 185-199. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4031777/
- Spoelstra-de Man, A. M., Elbers, P. W., & Oudemans-van Straaten, H. M. (2018). Making sense of early high-dose intravenous vitamin C in ischemia/reperfusion injury. Critical Care, 22 (1), 70. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5861638/
- Sinha, J., Das, N., & Basu, M. K. (2001). Liposomal antioxidants in combating ischemia-reperfusion injury in rat brain. Biomedicine & pharmacotherapy , 55 (5), 264-271. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/11428552
- Fritz, H., Flower, G., Weeks, L., Cooley, K., Callachan, M., McGowan, J., ... & Seely, D. (2014). Intravenous vitamin C and cancer: a systematic review. Integrative cancer therapies , 13 (4), 280-300. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/24867961
- Pullar, J., Carr, A., & Vissers, M. (2017). The roles of vitamin C in skin health. Nutrients , 9 (8), 866. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5579659/
- Suntres, Z. E., & Omri, A. (2006). The role of liposomal antioxidants in oxidative stress. In Nanocarrier Technologies (pp. 191-205). Springer, Dordrecht. Full text:
- Figueroa-Méndez, R., & Rivas-Arancibia, S. (2015). Vitamin C in health and disease: its role in the metabolism of cells and redox state in the brain. Frontiers in physiology , 6 , 397. Full text: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4688356/
- Meves, A., Stock, S. N., Beyerle, A., Pittelkow, M. R., & Peus, D. (2002). Vitamin C derivative ascorbyl palmitate promotes ultraviolet-B-induced lipid peroxidation and cytotoxicity in keratinocytes. Journal of investigative dermatology, 119 (5), 1103-1108. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/12445199
- Dr. Weil: Time for a change? https://www.drweil.com/vitamins-supplements-herbs/vitamins/vitamin-c-time-for-a-change/
- The Linus Pauling Institute: The Bioavailability of Different Forms of Vitamin C: https://lpi.oregonstate.edu/mic/vitamins/vitamin-C/supplemental-forms
- De Ritter, E., Cohen, N., & Rubin, S. H. (1951). Physiological availability of dehydro-L-ascorbic acid and palmitoyl-L-ascorbic acid. Science, 113 (2944), 628-631. Abstract: https://www.cabdirect.org/cabdirect/abstract/19511402702
- Cadeau, C., Fournier, A., Mesrine, S., Clavel-Chapelon, F., Fagherazzi, G., & Boutron-Ruault, M.C. (2016). Vitamin C supplement intake and postmenopausal breast cancer risk: interaction with dietary vitamin C. American Journal of Clinical Nutrition , 104 (1), 228-234. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/27194303
- Kiely, M.E., Lal, S., & Nair, N.P. (1987). Effect of ascorbic acid on brain amphetamine concentrations in the rat. Progress in neuro-psychopharmacology & biological psychiatry, 11 (2-3), 287-290. Abstract: https://www.ncbi.nlm.nih.gov/pubmed/3628833
- Cambridge Commodities - What is the Percentage of Vitamin C in Ascorbyl Palmitate? https://www.cambridgecommodities.com/ingredients/ingredient-view,ascorbyl-palmitate_2091.htm
- PubChem - Ascorbyl Palmitate - https://pubchem.ncbi.nlm.nih.gov/compound/Ascorbyl-palmitate
Source: https://coremedscience.com/blogs/wellness/how-to-pick-the-best-liposomal-vitamin-c